

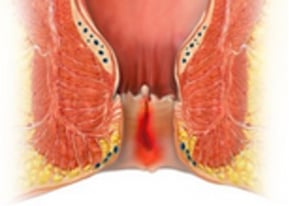
Anal Fissure
Occurring in young people with pain, blood and burning - during and after bowel movements.
| Facts about the Anal fissure operation |
|
Outpatient surgery: Yes |
|
General anesthesia: Yes |
| Operation time: 5 - 10 minutes |
| Open wounds: Yes, but small |
| Incapacity for work: 5 - 14 days |
|
Cost: Covered by Public health insurance. Laser therapy and Botox occurs additional costs. |
Anal fissures are small breaks in the very painful anal skin (anoderm), which are often caused by hard stools or strong pushing. The main symptom is burning pain during bowel movements and 1-2 hours afterwards.
As the anal fissure is a laceration, large amounts of blood can also be discharged. Patients often report a painful tearing of the anal skin. The pain can be so severe that patients avoid bowel movements and become constipated (proctogenic constipation), which worsens the situation. This starts a cycle that needs to be stopped.
We have extensive experience in the treatment of anal fissures, especially in young people, and always try to avoid surgery. However, if surgery is necessary, we perform it safely, painlessly and without complications.
A new feature is the combination with BOTOX or autologous blood (PRP) during surgery, which leads to a significant reduction in pain and faster wound healing. Don't be afraid and trust us.
Acute and Chronic Anal Fissures
A distinction must be made between the acute and chronic form of anal fissure, as the treatment is different. The definition is not entirely standardized.
Acute anal fissure: We see the acute form as a fresh tear with pain and blood that has the best chance of healing. The most important goal for good healing is a well-formed, regular and soft bowel movement. It is helpful to increase the amount you drink each day and, if necessary, to switch to a high-fiber diet. If this alone is not enough, stool regulators such as psyllium husks should be taken.
Creams that promote blood flow to the sphincter muscle, which leads to better wound healing, can be used to support this. Ointments with a local anaesthetic can also be administered. This often results in complete healing within a few days.
Anyone can develop an acute anal fissure in the course of their life. They occur more frequently in women after childbirth, for example, in combination with iron supplements or after anal sex.
Chronic Anal Fissure
Chronic anal fissure: If an anal fissure has been present for longer than 6 weeks, a clear change in the fissure has already occurred. The fresh tear has turned into a firm scar and the outermost part of the internal sphincter muscle is included in this process.
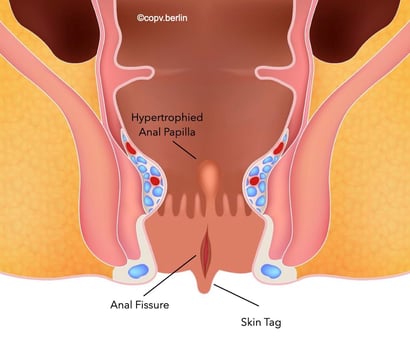
In addition, so-called secondary formations develop due to the chronic irritation.
These include the externally visible and palpable outpost fold, which is often misinterpreted as a hemorrhoid. This is a pure skin fold (mariscus). In the anal canal, a so-called hypertrophic anal papilla forms at the end of the anal fissure.
These are regular small protrusions from the mucous membrane that can grow up to 3 cm in size and then protrude from the anus.
Drug Therapy for Anal Fissures
If a fissure persists for several weeks, treatment with medication alone is initially indicated. An ointment with the active ingredient Diltiazem is usually used, as it has fewer side effects such as dizziness and headaches. This therapy can last up to 3 months and in many cases leads to a cure. However, secondary formations that have already developed, such as the outpost fold or the hypertrophic anal papilla, remain. Only surgery can help here.
If the pain is very severe and an examination is not possible, a diagnostic procedure under anesthesia is often necessary to rule out a malignant cause of the symptoms. This can easily be done on an outpatient basis. If the diagnosis of a chronic anal fissure is confirmed, surgical treatment can be carried out in the same session. We recommend the additional administration of Botox for faster and less painful healing.
Please note: The prescription with e.g. diltiazem, isorbide dinitrate or glycerol trinitrate is not covered by the statutory health insurance companies (AOK, Barmer, TK...). You have to pay for these prescriptions, which cost between 25€ and 30€, yourself and will not be reimbursed by your health insurance company.
This is why the prescriptions are printed on a green private prescription and not on a pink prescription. This is not an oversight on our part, even if the pharmacy claims it is.
Botox Therapy for Anal Fissure
Significant improvement in surgical results for anal fissures with less pain and faster wound healing
Botulinum toxin A is a powerful neurotoxin which is considered to be the cause of botulism.
The toxin inhibits the transmission of excitation from the nerve cells to the muscle, causing the muscle strength to weaken or fail completely for a certain area, depending on the dosage of the toxin.
"Botox leads to a significant improvement in surgical results for anal fissures with less pain and faster wound healing"
Botox is now used in various areas of medicine. Mainly in aesthetic medicine, where, for example, the fine facial muscles are partially paralyzed, causing the skin to smooth out and wrinkles to disappear. The treatment of armpits or hands is also known to reduce perspiration.
With all therapies, however, it should be borne in mind that the Botox is broken down by the body after several monthsand the effect wears off. For this reason, six-monthly treatments are common in aesthetic medicine.
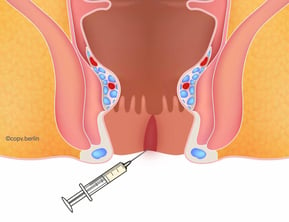
The situation is slightly different for anal fissures, but the therapeutic effect is similar. Patients with a chronic anal fissure, i.e. one that has been present for a long time, generally have higher muscle pressure in the internal sphincter muscle. This leads to a lack of blood flow and subsequent wound healing disorders.
The botulinum toxin injection immobilizes a small part of the sphincter muscle for 4-6 months, allowing the wound to heal calmly and painlessly due to the improved blood flow.
The Botox begins to take effect after three days and 75% of patients experience a significant improvement in pain symptoms within the first week. According to the literature, the remission rate after a therapeutic session is around 80%, in our own experience it is over 90%. It is not necessary to repeat the injection.
What needs to be considered afterwards?
The effect usually sets in after a few days and the maximum muscle paralysis appears after 4-7 days. After 4-6 months, the effect of the paralysis diminishes and muscle activity is completely restored.
Side effects such as bleeding, bruising and infections are very rare. The only undesirable side effect is anal incontinence, i.e. the inability to hold out diapers and stool. The risk of (temporary) minor incontinence is increased with weak muscle pressure and in women of advanced age and after several deliveries.
However, if incontinence occurs, the rate is less than 5% and lasts for about 2 weeks. The main symptoms are involuntary leakage and smearing of stool. Patients are not able to hold their stool with the usual dosage.
Important: This is a so-called "off label ” therapy. Botox is therefore not approved as an official medication for the treatment of anal fissures and is therefore not covered by statutory health insurance. It is an IGeL service that we usually use during an operation under anesthesia. However, it can also be used as an alternative to Diltiazem ointment. However, not every patient is suitable for this form of therapy.
Patients with private insurance should clarify with their insurance company whether the costs will be covered before the operation. Complications or major side effects are not to be expected.
"Botox can be used safely as a treatment option with or without surgery"
FAQ about Botox therapy in Anal fissures
Botox relaxes the internal sphincter muscle. Many anal fissures do not heal because the muscle is tense and blood flow to the wound is greatly reduced. Temporary relaxation reduces pain, lowers pressure, and allows the fissure to heal undisturbed.
The injection is usually performed on an outpatient basis. Local anesthesia or very light sedation is usually used. The procedure itself takes only a few minutes. Most patients report at most a brief feeling of pressure or a prick. Nevertheless, we recommend combining the injection with surgery.
Muscle relaxation typically begins after 3–7 days and reaches its full effect after about 2 weeks. Botox lasts for approximately 3–5 months. During this period, the fissure can heal completely in most patients.
Side effects are rare overall. Possible side effects include: slight burning or bleeding at the injection site, temporary slight stool smearing or reduced sphincter strength (usually mild and temporary), and very rarely infections or allergic reactions. Permanent incontinence is extremely rare, as Botox loses its effect completely.
Botox is particularly suitable for chronic anal fissures when ointments and other conservative measures are no longer sufficient. Surgery (excision of the fissure/laser therapy) may be considered if: the fissure does not heal despite Botox, there is very severe muscular hypertension, or there are long-standing, deep, or complicated fissures with scarring. However, in quite a few patients, the fissure heals with Botox without surgery.
We can only determine this after an examination at our clinic. If patients are in severe pain or are very sensitive, Botox should only be administered under general anesthesia. Botox should not be administered to pregnant or breastfeeding women.
Botox is still an expensive medication and is not covered by health insurance for the treatment of anal fissures. The cost is therefore between €250 and €350, depending on the preparation.
PRP - Platelet-rich plasma therapy for anal fissures
Autologous blood as a new therapeutic method for improved wound healing in anal fissures
| PRP Check |
| Hospital stay: No, outpatient treatment in combination with anal fissure operation |
| Number of treatments: For anal fissures, only one treatment during surgery |
| Incapacity for work: No, not because of PRP therapy. |
|
General anaesthesia: As part of the operation, yes |
|
Costs: Approximately €200–€400 per session |
"Autologous blood therapy can be used to great effect in anal fissure surgery to achieve faster and optimal wound healing"
Our blood consists of water, white and red blood cells, and platelets.
In PRP (Platelet-Rich Plasma) therapy, a protein-rich concentrate is extracted from the platelets and injected into the relevant area of the body using a special syringe.
Platelets contain numerous growth factors and cell messengers (cytokines) that promote cell renewal, giving PRP treatment its regenerative potential and stimulating growth in the surrounding tissue.
How does autologous blood therapy (PRP) work?
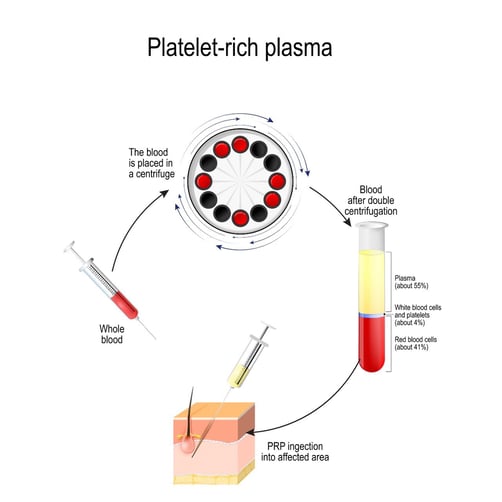
After the blood sample has been taken, the whole blood is immediately placed in a special tube in a centrifuge. No further processing is necessary. Centrifugal force separates the blood into three components. This occurs due to the different specific weights.
The top layer consists of plasma, which is low in blood cells and platelets and accounts for approximately 55% of the total volume. The middle layer contains white blood cells (leukocytes) and platelets (thrombocytes), which make up approximately 4% of the total volume. The bottom layer consists of red blood cells (erythrocytes), which clump together to form a blood clot and make up approximately 41% of the total volume.
The platelet-rich plasma is drawn from the tubes and injected into the patient's body at the site to be treated, where the added growth factors initiate tissue growth and improve healing.
Treatment should not be carried out on patients with tumors, during pregnancy, or during therapy with Marcumar or similar blood thinners.
"PRP therapy is a useful attempt to stimulate wound healing when other measures are ineffective"
Advantages of treatment with autologous PRPAdvantages of treatment with autologous PRP
- Minimally invasive therapy
- Hardly any side effects, as the patient's own blood is used without additives
- No local anesthesia
- Outpatient treatment
- Long-lasting effects
- Short treatment times (10 minutes)
FAQ - Frequently asked questions about the new PRP therapy for anal fissures
PRP (“platelet-rich plasma”) is a concentrate of platelets and growth factors obtained from the patient's own blood. These growth factors promote tissue regeneration, improved blood circulation, and accelerated wound healing. In the case of an anal fissure, PRP supports the natural healing process of the mucous membrane and can significantly reduce pain and healing time.
First, a small amount of blood (10 ml) is taken and processed in a centrifuge. The concentrated PRP is then injected into the area of the fissure or applied locally, depending on the method. Due to the amount and the very sensitive region around the anus, we only perform this therapy as part of an operation under general anesthesia. The injection is therefore painless. However, slight muscle pain may occur afterwards, similar to “muscle soreness.”
Many patients notice an improvement in pain within just a few days. Due to the anesthesia, we only perform one session, but this can be repeated as often as desired.
Since PRP is produced from the patient's own blood, it is very well tolerated. Possible, mostly harmless side effects include: slight pain or pressure at the injection site, temporary swelling, and very rarely, infections. Allergies are practically impossible. The method is considered safe.
PRP is often used for: chronic anal fissures that heal poorly. Patients who want to avoid Botox or surgery Fissures that do not heal despite ointments and stool regulation. PRP is less suitable for: acute infections, deep-seated fistula tracts severe spasm of the sphincter muscle (Botox may be more appropriate here). Fissures that persist despite PRP → surgery may then be necessary.
The therapy costs between €300 and €350 per session. The costs are not covered by statutory health insurance. Privately insured patients should ask their insurance company in advance whether they will cover the costs.
Laser Therapy for Anal Fissure
Laser Fissure Cleaning (LFC) - a new treatment for anal fissures
In gentle laser therapy (LFC), the fissure is obliterated with particular precision using targeted heat.
The penetration depth and damage to the internal sphincter muscle is very low, which leads to significantly less pain in the healing phase.
The advantages
- The risk of incontinence is greatly minimized.
- The treatment is generally perceived as very painless.
- Severe scarring is avoided to a large extent.
- The risk of infection is significantly reduced due to the reduced trauma.
In the classic anal fissure, there is a deeper wound (ulcer) with so-called secondary formations such as the outpost fold (mariscus) and the hypertrophic anal papilla inside.
These structures must be removed for new and firm wound healing. Until now, this has only been possible by excision, which damages the neighboring structures due to the depth of penetration, resulting in increased pain.

In laser therapy, the fissure is irradiated with the diode laser and precisely removed thanks to the exact setting. The sphincter muscle is optimally protected and the risk of incontinence is reduced to a minimum compared to conventional methods.
Due to the low penetration depth of the light beam, laser therapy is generally painless and places little strain on the body. Due to the precise working method, no larger and deeper wounds occur. The fissure can heal faster and more safely.
"With laser therapy, anal fissures can be removed with extreme precision. The laser ensures ideal hemostasis and a minimal wound surface, so that patients receive the gentlest possible treatment"
Important: Unfortunately, laser therapy is not yet covered by statutory health insurance. We can therefore only offer this surgical procedure as a self-pay service.
You are welcome to contact us for a cost estimate.
Privately insured patients must clarify the cost coverage with their health insurance company before the operation.
You are welcome to book an appointment with our doctors.
We look forward to hearing from you.